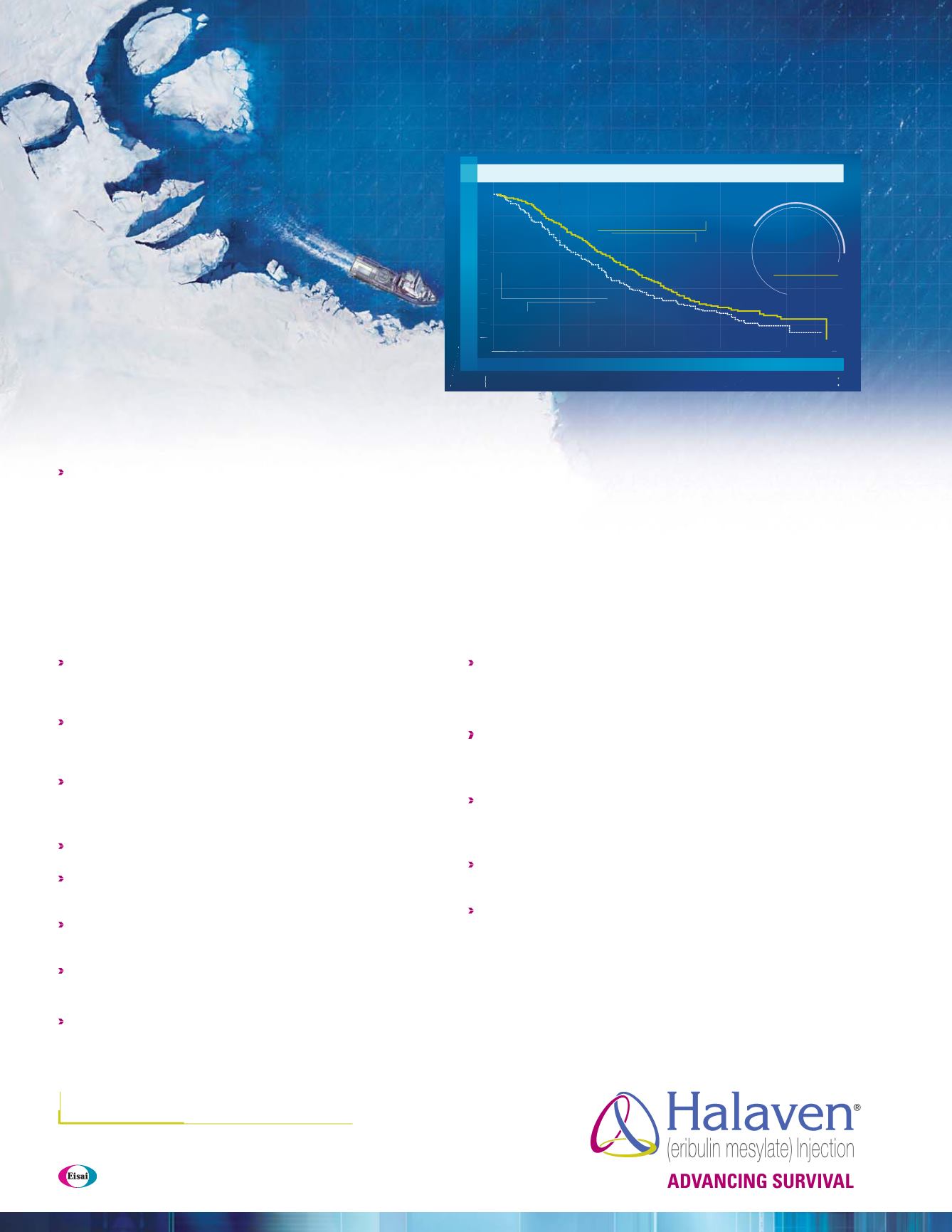
UPDATEDOVERALLSURVIVAL (OS)ANALYSIS (UNPLANNED):
MEDIANOS,MONTHS (95%CI)
1,2,a
1.0
0.9
0.8
07
.
0.6
0.5
0.4
0.3
0.2
0.1
0.0
T
reatment of
P
hysician’s
C
hoice
(n=254)
10.6
(9.2, 12.0)
Deaths
=203
Halaven
(n=508)
13.2
(12.1,14.4)
Deaths
=
386
TIME (MONTHS)
PROPORTION OF PATIENTS ALIVE
0
6
1
2
18
24
30
36
508
406
274
142
54
11
0
254
178
106
61
26
5
0
Halaven
TPC
Number of
patients at risk
25%
(2.6 month)
INCREASE
IN MEDIAN OS
HALAVEN
®
is a registered trademark used by Eisai Inc.under license from Eisai R&D Management Co.,Ltd.
© 2013 Eisai Inc. All rights reserved. Printed in USA/November 2013 HALA0480
Important Safety Information
Neutropenia
Monitor complete blood counts prior to each dose, and increase the frequency
of monitoring in patients who develop Grade 3 or 4 cytopenias. Delay
administration and reduce subsequent doses in patients who experience
febrile neutropenia or Grade 4 neutropenia lasting longer than 7 days
Severe neutropenia (ANC <500/mm
3
) lasting more than 1 week occurred in 12%
(62/503) of patients. Patients with elevated liver enzymes >3 × ULN and bilirubin
>1.5 × ULN experienced a higher incidence of Grade 4 neutropenia and febrile
neutropenia than patients with normal levels
Grade 3 and Grade 4 neutropenia occurred in 28% and 29%, respectively, of
patients who received Halaven. Febrile neutropenia occurred in 5% of patients
and two patients (0.4%) died from complications
Peripheral Neuropathy
Patients should be monitored closely for signs of peripheral motor and
sensory neuropathy
Grade 3 peripheral neuropathy occurred in 8% of patients, and Grade 4 in
0.4% of patients who received Halaven. Delay administration of Halaven until
resolution to Grade 2 or less
Neuropathy lasting more than 1 year occurred in 5% of patients. Twenty-two
percent of patients developed a new or worsening neuropathy that had not
recovered within a median follow-up duration of 269 days (range 25-662 days)
Peripheral neuropathy (5%) was the most common adverse reaction resulting
in discontinuation
Pregnancy Category D
Halaven is expected to cause fetal harm when administered to a pregnant
woman and patients should be advised of these risks
QT Prolongation
In an uncontrolled ECG study in 26 patients, QT prolongation was observed
on Day 8, independent of eribulin concentration, with no prolongation on
Day 1. ECG monitoring is recommended for patients with congestive heart
failure; bradyarrhythmias; concomitant use of drugs that prolong QT interval,
including Class Ia and III antiarrhythmics; and electrolyte abnormalities
Correct hypokalemia or hypomagnesemia prior to initiating Halaven andmonitor
electrolytes periodically during therapy. Avoid in patients with congenital long
QT syndrome
Hepatic and Renal Impairment
For patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic and/
or moderate (CrCl 30-50 mL/min) renal impairment, a reduction in starting dose
is recommended
Most Common Adverse Reactions
Most common adverse reactions (≥25%) reported in patients receiving Halaven
were neutropenia (82%), anemia (58%), asthenia/fatigue (54%), alopecia (45%),
peripheral neuropathy (35%), nausea (35%), and constipation (25%)
The most common serious adverse reactions reported in patients receiving
Halaven were febrile neutropenia (4%) and neutropenia (2%)
References: 1.
Halaven [package insert]. Woodcliff Lake, NJ: Eisai Inc; 2013.
2.
CortesJ,etal.
Lancet
.
2011;377(9769):914-923.
3.
Saad ED, et al.
J Clin Oncol
. 2010;28(11):1958-1962.
4.
Slamon DJ, et al.
N Engl J Med.
2001;344(11):783-792.
5.
Geyer CE, et al.
N Engl J Med
. 2006;355(26):2733-2743.
6.
von Minckwitz G, et al.
J Clin Oncol
. 2009;27(12):1999-2006.
7.
Miller K, et al.
N Engl J Med
.
2007;357(26):2666-2676.
8.
Robert NJ, et al.
J Clin Oncol
. 2011;29(10):1252-1260.
9.
Sparano JA, et al.
J Clin Oncol
. 2010;28(20):3256-3263.
CI=confidence interval; MBC=metastatic breast cancer.
a
Conducted in the intent-to-treat population.
Results from an updated, unplanned survival analysis of the Phase III, randomized, open-label, multicenter,
multinational
E
isai
M
etastatic
Br
east Cancer Study
A
ssessing Physician’s
C
hoice versus
E
7389 (Eribulin)
(EMBRACE) trial of Halaven versus
T
reatment of
P
hysician’s
C
hoice (TPC) in patients with MBC (N=762),
conducted when 77% of events (deaths) had been observed. The primary endpoint was OS. Patients were
randomized (2:1) to receive either Halaven 1.4 mg/m
2
intravenously for 2 to 5 minutes on Days 1 and 8 of
a 21-day cycle, or any single-agent therapy, selected prior to randomization. At baseline, all patients had
received ≥2 prior chemotherapeutic regimens for metastatic disease and demonstrated disease progression
within 6 months of their last chemotherapeutic regimen. All patients received prior anthracycline- and taxane-
based chemotherapy, unless contraindicated. Therapies in the TPC arm consisted of 97% chemotherapy (26%
vinorelbine, 18% gemcitabine, 18% capecitabine, 16% taxanes [included paclitaxel, docetaxel, nab-paclitaxel,
and ixabepilone], 9% anthracyclines, 10% other chemotherapy), and 3% hormonal therapy.
GIVE
your patients an
opportunity for
MORE LIFE
The
FIRST
and
ONLY
single agent
that significantly extended
OVERALL
SURVIVAL
in third-line MBC
1,3-9
The updated OS analysis was
consistent with the primary analysis
1
The primary analysis, conducted when ~50% of events (deaths)
had been observed, demonstrated a median OS for Halaven vs TPC
of 13.1 months (95% CI: 11.8, 14.3) vs 10.6 months (95% CI: 9.3, 12.5),
hazard ratio=0.81 (95% CI: 0.66, 0.99) (
P
=0.041)
1,2
Visit
Please see accompanying brief summary of Halaven full Prescribing Information.
Indication
Halaven is indicated for the treatment of patients with metastatic breast cancer who have previously received at least two chemotherapeutic regimens for the
treatment of metastatic disease. Prior therapy should have included an anthracycline and a taxane in either the adjuvant or metastatic setting.


